The Concept of Risk-Weighted Impact (RWI):
The goal of the RWI approach is to reframe risk-assessment from comparing the probability of negative events (“How likely is a complication to occur?”) to comparing the impact on the patient of such an event (“How many years of life are impacted from a possible complication?”).
All calculators on this website compare these two risk-assessment approaches: 1) the cumulative lifetime event risk approach, 2) the RWI approach.
Outputs:
Total probability of an event occuring during a person's lifeOutputs:
Risk-weighted number of years impacted by a possible event occuringInputs:
- Event probabilities
- Life expectancy
Inputs:
- Event probabilities
- Life expectancy
- (Optional) Health-related Quality of Life Measure
When comparing two treatments with risks that take place at the same time (i.e. two surgical options), there is not a difference between these two risk-assessment approaches. But there can be a large difference when comparing treatments that have risks that occur over different time horizons.
This is important because time is a major factor for the impact of a risk. This can illustrated with a hypothetical: if you were going to be struck by a car and killed, would you prefer it happen when you’re 35 or 75 years old? If your life expectancy were 80, you’d lose 45 years of life if it occurred earlier rather than 5 years of life if it occurred later. Generally, impact of an event is lessened the later it occurs (fewer years of life are impacted).
Only considering cumulative lifetime event risk does not take this time factor into account, while the RWI approach does. This is important when considering treatments with risks occurring over different timeframes, most commonly between an intervention with upfront risk and the distributed risk of the natural history of the disease.
To see how each approach is calculated and how they differ, consider the following simplified example:
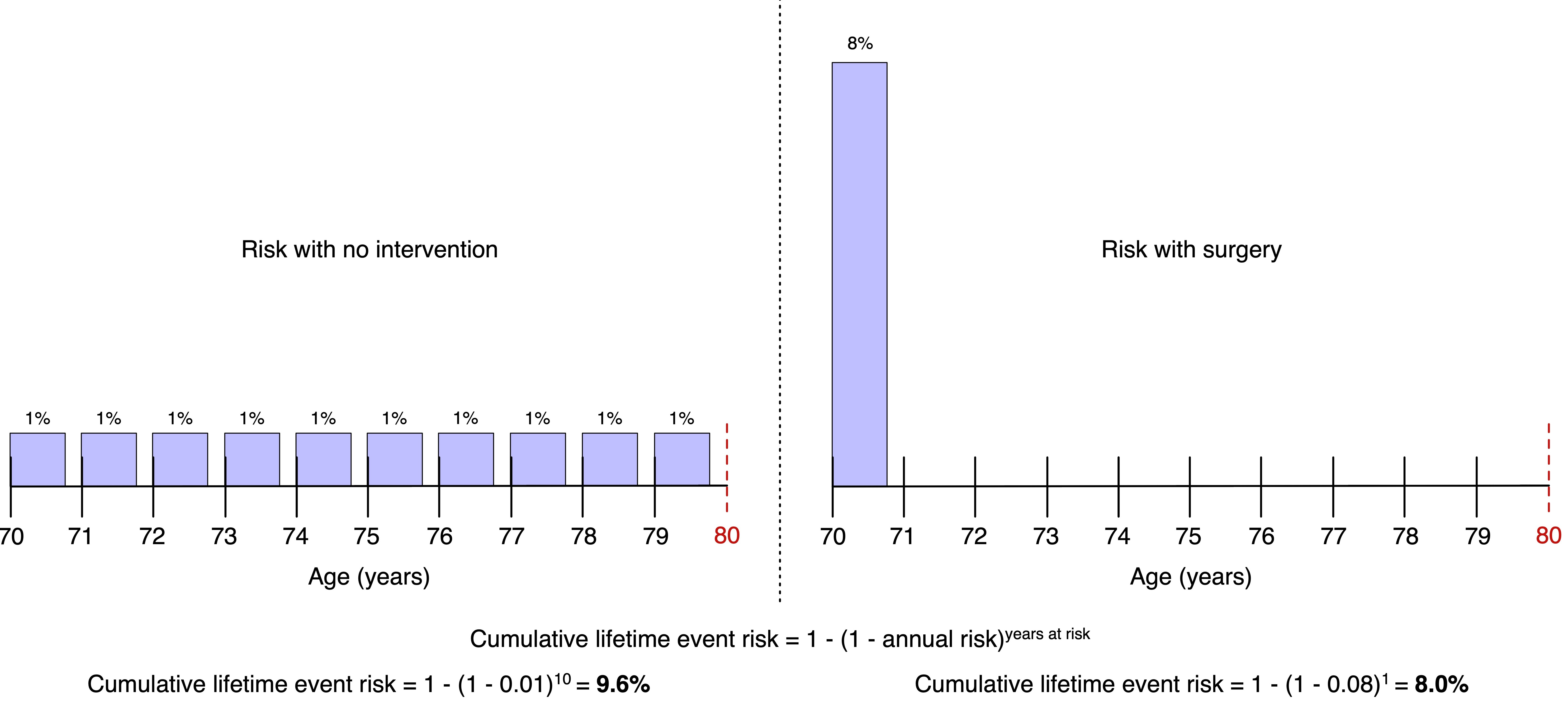
A 70-year-old man with a life expectancy of 80 years old was diagnosed with a disease that has a 1% chance of killing him each year. There is a surgical treatment that would cure him but comes with an 8% risk of dying from the intervention. Should he pursue the surgery or not?
Using cumulative lifetime event approach, the risks of dying from surgery (8%) appear favorable to the risk of dying from the untreated disease (9.6%). But it can be appreciated that all the risk for surgery is incurred upfront while the risk of the disease is spread out over the remaining 10 years of his life.
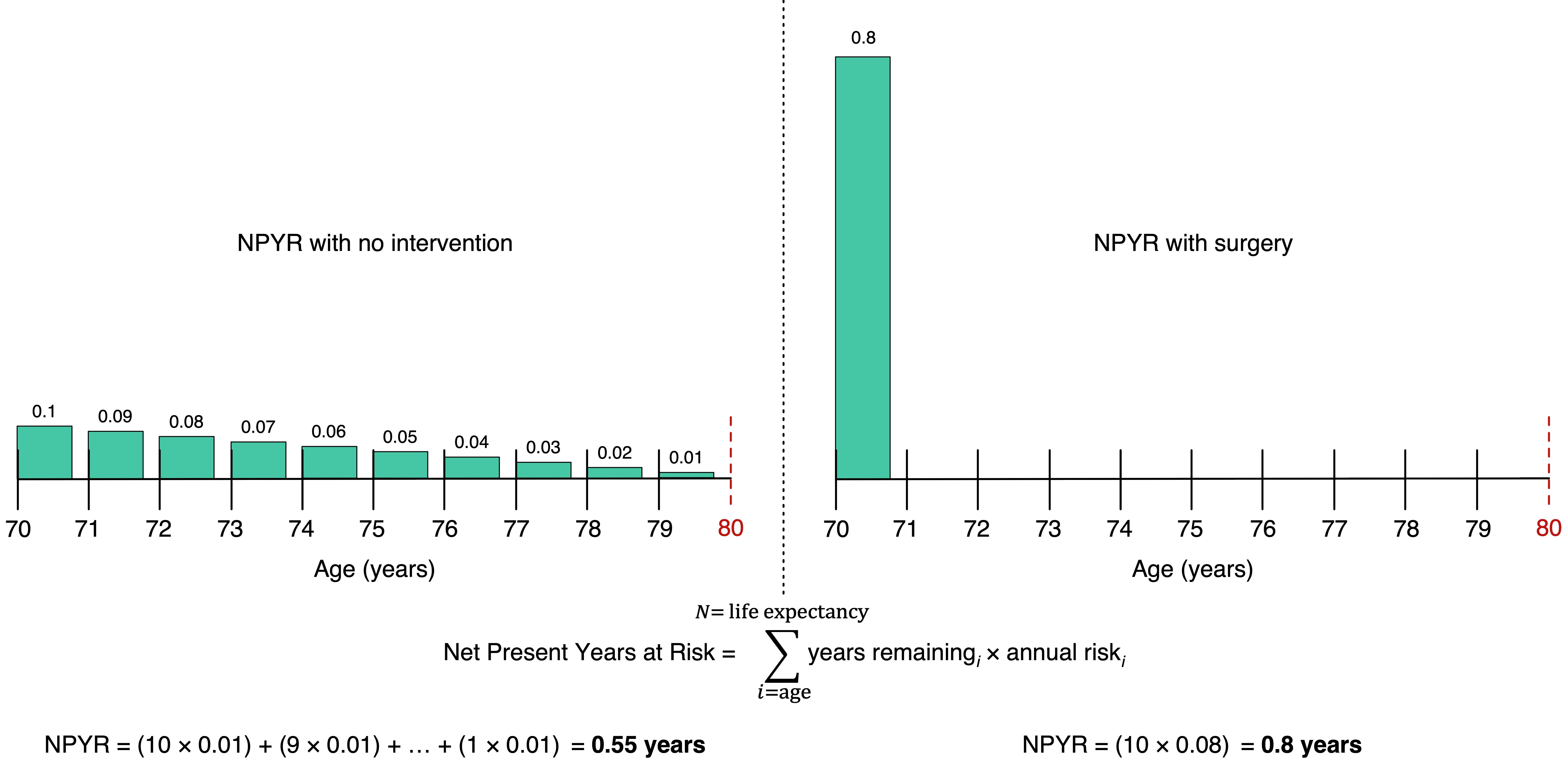
Given these different risk distributions, it is worth considering the impact of these risks using the RWI approach. When looking at the average number of years lost, the surgical treatment is actually riskier (0.8 years of life lost compared to 0.55 years). This is because the entirety of the risk is incurred upfront and there is an 8% chance that he could lose all 10 remaining years instead of the disease risk of 1% per year (so 1% chance of losing the same 10 years, but also 1% chance of losing the last year only).
Number to Beat:
To make RWI more actionable, the “number to beat” can be calculated based on comparison of the risk of an alternative, such as observation alone. The number to beat is the initial treatment risk that results in an equivalent RWI for that patient. This enables a clinician considering an intervention to evaluate the maximum upfront risk for the treatment to be of equal or lower risk to an alternative treatment approach.
For the simplified example above, surgery would need to result in an RWI of 0.55 years or less. This would occur with an upfront surgical risk of 5.5% or less, meaning the “number to beat” is 5.5%.
Assumptions and Limitations:
An important assumption when using these risk calculators is that the risks are equivalent. In the above simplified example, the risk was the same (death), but real-world risks include a variety of complications that cause a variety of disabilities, making comparing risk probabilities challenging.
Most importantly, it is essential to recognize that risk-assessment is multifactorial and complex. Recommendations about treatments must be based on expert clinical judgement and consideration of individual patient preferences and values. Clinical data is often limited or absent, and clinician judgement based on experience is required to attempt to fill such gaps. The RWI approach and calculators are only tools to assist in such complex decisions and do not attempt to define optimal choices.
For more detailed information on the RWI approach, calculating risks, and full Python code repository, see Publication section for a link to the companion peer-reviewed publication.